Aim: Lowering systolic blood pressure (SBP) to <120 mmHg has been shown to reduce cardiovascular events and mortality. Whether this should be the target is controversial. We therefore studied the relationship between SBP attained and outcome using network meta-analysis.
Methods: We searched for randomised trials comparing different SBP targets. The mean SBP attained was classified into five groups (110–119, 120–129, 130–139, 140–149 and 150–159 mmHg). The outcome variables analysed using R were major adverse cardiovascular events (MACE), cardiovascular mortality, stroke and MI.
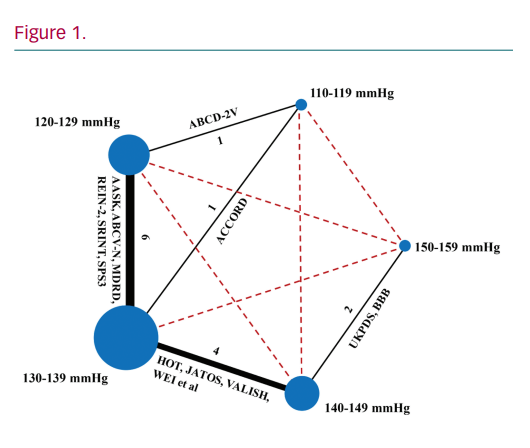
Results: 14 trials with a total of 4,4015 patients were included (Figure 1). Lowering SBP to 120–129 mmHg significantly reduced stroke and MACE when compared to 130–139 mmHg (OR 0.83, 95% CI [0.69–0.99] and 0.84, 0.73–0.96), 140–149 mmHg (0.73, 0.55–0.97 and 0.74, 0.60–0.90), and 150–159 mmHg (0.43, 0.26–0.71 and 0.41, 0.30–0.57), respectively. The risk of stroke was further lowered with more intensive control to <120 mmHg (0.58, 0.38–0.87, 0.51, 0.32–0.81, and 0.30, 0.16–0.56, respectively). In contrast, the risk of cardiovascular mortality and MI was significantly higher with SBP ≥150 mmHg when compared to 120–129 mmHg (2.18, 1.32–3.59 and 1.73, 1.06–2.82) and 130–139 mmHg (1.71, 1.11–2.61 and 1.53, 1.01–2.32).
Conclusion: Lowering SBP to <130 mmHg reduces MACE and stroke. Further lowering to <120 mmHg can reduce stroke if the treatment is tolerated. Long-term SBP should not exceed 150 mmHg because of the increased risk of cardiovascular events and death.